At the London Orthotic Consultancy, we have treated adult patients with scoliosis ranging from the age of 30 up to 87.
Scoliosis in adults can be broadly separated into two categories; adult idiopathic scoliosis and adult degenerative scoliosis. However, a person can experience both at the same time.
Factors that can aggravate scoliosis in later life include:
‘Idiopathic’ describes a condition that arises spontaneously without a known cause. Adult idiopathic scoliosis is often a continuation of adolescent idiopathic scoliosis; when the spine begins to curve before or throughout teenage years. Curves can increase by 0.5° to 2° per year.
Adult scoliosis is often aggravated by ageing which naturally causes the spinal discs and joints to degenerate. Some adults will overcompensate by leaning forward to alleviate the pressure of the spine collapsing into the spinal nerves which then worsens the overall stability and equal loading of the spine. The rate of progression is between 5° and 10° per decade, or around 1% per year (which is significantly less than in children and adolescents).
Symptoms: rib hump, shoulder asymmetry, stiffness, lower back pain, pain or pins and needles in the legs caused by pressure on the nerves.

Also called de novo scoliosis – or ‘new’ scoliosis – this form of the condition is actively caused by the degeneration of the spinal discs and joints and typically affects the lower back. The degeneration of the spine causes pain in the lower back and the curve to form.
Symptoms: rib hump, shoulder asymmetry, stiffness, lower back pain, pain or pins and needles in the legs caused by pressure on the nerves, loss of sagittal balance.
For adults, treatment concentrates on helping alleviate specific symptoms. For this, it’s important to ask what the main concern is: is it pain? Is it appearance? Is it a hip sticking out to the side or the rib hump appearance? Once it has been established which symptoms the patients want us to concentrate on, an appropriate method of treatment can be decided with the patient being offered the team’s opinion and possible outcomes for their individual case.
Postural advice and training are the first-line treatment for adults with scoliosis. Posture is the priority as an adult’s gravity is not generally kind to the spine.
The majority of adults suffering from scoliosis will not require spinal surgery. Spinal surgery is a major procedure and carries potentially serious complications and risks. Therefore, it is normally reserved for very serious cases, i.e. if the curve is getting significantly worse affecting breathing or the nerves in the spine are being pinched under the pressure and causing serious pain.
At the London Orthotic Consultancy, we brace adults depending on what their needs are.
As adults have reached skeletal maturity – when the vertebrae are no longer malleable – an orthotic brace is not likely to straighten the spine (reduce the Cobb angle), like in adolescence.
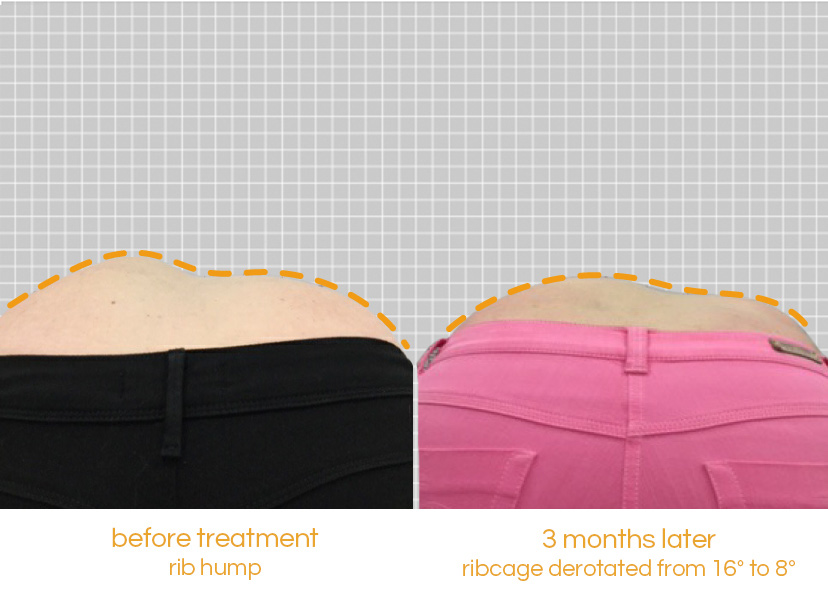
A brace can be used to reduce posture-related pain (avoiding medication or surgery) or improve aesthetics, appearance and posture at a quicker pace. We do brace severe scoliosis in adults to prevent surgery and re-surgery due to curve progression, especially when curves are large and difficult to treat with exercises and postural advice alone.


“It’s life-changing, my swimming coach has even remarked what a difference my treatment has made" Read how pectus bracing treatment helped to correct Aris' complex chest deformity, involving a combination of pectus excavatum, pectus carinatum and rib flaring.

Cerebral palsy patient Lucas sees significant improvement in his walking after only six months in his new custom Ankle Foot Orthoses (AFOs), designed by Professor Saeed Forghany in our Manchester clinic. Hear how a detailed gait analysis and bespoke AFOs significantly improved Lucas's gait and comfort.

Freddie’s positional plagiocephaly was treated successfully with the LOCBand Lite, going from 11mm to 2mm after four months in his helmet.

Adult club foot (talipes) patient Natasha says, "I cannot stress how amazing my AFOs are and how they have changed so much for me. The support they give me allows me to walk without crutches outside the house for the first time in over fifteen years."

Diagnosed with adolescent idiopathic scoliosis at 14 years old, Polly and mum Zoe looked to the LOC Scoliosis Brace to help her curve and avoid surgery at a later date.

LOC opens its first clinic in Northern Ireland, LOC Belfast, offer non-surgical orthotic treatment for scoliosis, pectus carinatum and pectus excavatum. Here, we will also be able to provide orthotic treatments for a range of adult and paediatric lower limb conditions including cerebral palsy, spina bifida, hypermobility, stroke, post-polio syndrome, and multiple sclerosis.

Mum Natalie shares her experience of having both her identical twins diagnosed with craniosynostosis. Ella and Nina had surgery at Great Ormond Street Hospital before going through cranial remoulding therapy at the London Orthotic Consultancy.

See how a thorough gait analysis and a correctly-fitted, bespoke Reciprocating Gait Orthosis (RGO) helped Ted, a spinal surgery and cancer survivor, improve his rehabilitation and mobility goals, getting him back on his feet again.