Pectus carinatum, also known as 'pigeon chest' is a congenital deformity of the anterior chest wall, and occurs when the breast bone is pushed outward by an abnormal overgrowth of cartilage.
Pigeon chest affects around one in 1,500 people and is slightly less common than pectus excavatum. It is present at birth but often becomes more noticeable in early adolescence when the ribcage and the rest of the body undergo growth spurts during puberty. Often both sides of the ribs are affected but in other cases, it can appear asymmetrical with one side worse than the other.
Pectus carinatum can also appear as part of another condition like scoliosis but is also associated with rarer musculoskeletal syndromes like Marfan syndrome.
Using a brace like the Dynamic Chest Compressor has become accepted as a first-line treatment for pectus carinatum. Orthotic bracing is proven to be a safe and effective way to provide successful outcomes without surgical intervention.
For further reading see this peer-reviewed article in Society Spotlight, a monthly overview of clinical papers from the societies of the American Academy of Orthotists and Prosthetists.
For patients considering LOC’s non-surgical treatment for pectus carinatum, we offer a free virtual consultation. During this, one of our specialist clinicians will give a detailed explanation of our treatment programme, discuss your individual symptoms and assess your suitability for treatment.
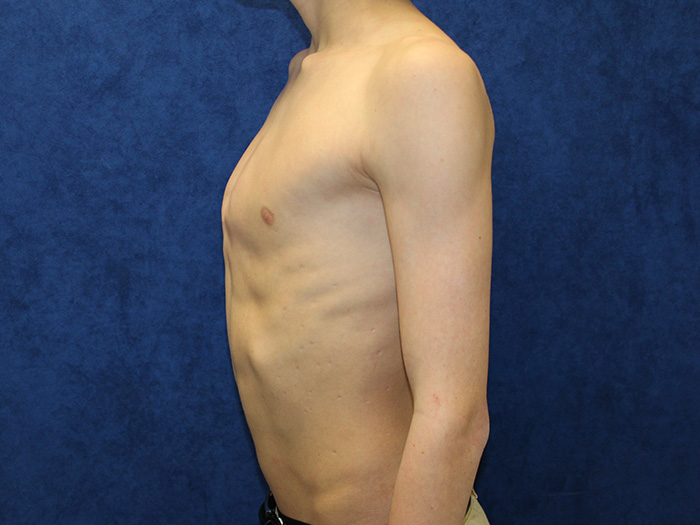
The exact cause of pectus carinatum is unknown, though it’s largely attributed to abnormal cartilage overgrowth between the bony ribs and the breast plate, causing the sternum – the breastbone – to buckle outwards (when it buckles inwards, this is referred to as pectus excavatum).
It is thought to be linked to hereditary as patients with pectus deformity usually have family members with the same condition. According to the American Board of Family Medicine about 40% of pectus patients have family members with a pectus condition but a genetic link is yet to be fully identified. For more information, head to our Causes page.
The breast bone protrudes out of the chest, causing it to bow out. Sometimes patients can suffer from a mixed deformity, half in and half out, so the chest appears asymmetrical.
Many who have pectus carinatum do not experience any further symptoms outside of their appearance. Some develop other associated complications listed below.
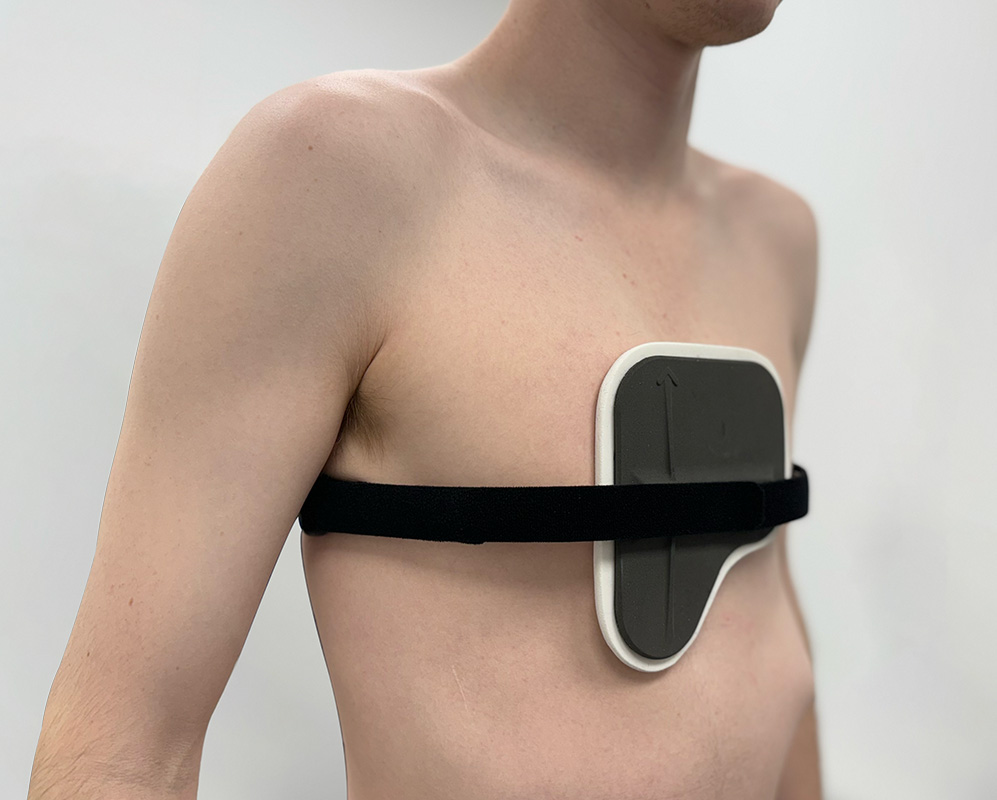
Pectus carinatum patient wearing the Dynamic Chest Compressor brace
An important aspect of having a pectus deformity is the reduced self-esteem that often accompanies it. While some people accept the shape of their chest, for others it can be traumatic; causing anxiety, negative self-image, low self-confidence and increased self-consciousness.
Research consistently shows that pectus carinatum often has a negative effect on a person’s ability to interact with others, and is a compelling reason for many to seek corrective help. In a 30 year, Californian study carried out by UCLA School of Medicine, the most common complaint from young patients was related to the unattractive physical appearance of the condition. In many cases, the cosmetic concerns and psychological effects are enough to warrant the need for treatment.
Many affected patients have no other physical symptoms, others may develop respiratory problems, some develop rigidity of the chest wall with decreased lung compliance or increased frequency of respiratory tract infections*
As a person gets older, the chest becomes more rigid and results are sometimes harder to achieve. The chest is more malleable in adolescents and children and tends to get stiffer as the skeleton matures.
Patients with pectus carinatum who comply with the required exercises will respond well to orthotic bracing, and there are normally two phases; one initial phase until correction is achieved and the next phase for maintenance, during which the brace is only worn at night.
Our non-surgical pectus treatment for pectus carinatum involves wearing a bespoke brace, the Dynamic Chest Compressor, combined with a programme of Yoga exercises that have been developed specifically to augment our treatment.
The dynamic chest compressor brace applies constant pressure over the area of the chest that needs to be remodelled. Because pectus carinatum is caused by the chest protruding, we use a bespoke brace that fits over the apex of the chest to push it in.
In cases where the ribs protrude as well, a separate, lower brace for rib flaring may be needed. As you push in the upper chest, the ribs tend to flare out so we use this lower brace to push the ribs back in.
It is over a decade since we introduced this new treatment for pectus carinatum, and we are building up ever more convincing, successful case histories. The most important factor in achieving a good result is compliance to the treatment programme and regular reviews preferably in the clinic, or via virtual consultations.
The length of treatment varies according to the age of the patient, the elasticity of the chest and the severity of the pectus carinatum. All pectus braces and treatments are tailored bespoke to each individual’s needs.

We offer free online pectus excavatum and pectus carinatum consultations via Skype, Facetime or Zoom for those worried about their chest shape.
Our treatment programme will be explained in detail so you can see whether treatment is right for you.

LOC's non-surgical treatment for pectus involves the Dynamic Chest Compressor, a custom made orthosis designed for an individual’s anatomy to specifically treat their particular type of pectus. For Pectus Excavatum patients we also prescribe the Vacuum Bell - it works by using a silicone cup and a vacuum pump to create an area of low pressure over the sunken part of the chest.
We manufacture bespoke braces for each patient, ensuring comfort and ease of compliance during treatment.

The London Orthotic Consultancy has been providing non-surgical pectus treatment since 2010 achieving positive results in our patients.
We are proud to be the pioneers of this treatment in the UK and are happy to share some patient successes for those who have undergone Pectus Carinatum treatment with us.

LOC director and pectus specialist, Sam Walmsley, has recorded a series of videos answering our client's frequently asked questions about our pectus treatments and exercise programmes.
For patients who want to avoid surgery, non-surgical pectus treatment can be a great way to achieve a flatter chest, but often, patients are unsure of what treatment involves.

We offer orthotic treatment for international patients seeking non-surgical pectus excavatum and pectus carinatum bracing in the UK. Our specialist clinicians have extensive experience treating pectus deformity patients from around the world.
We regularly treat international patients with our evidence-based orthotics including those from Europe, South America and the Middle East.

LOC's pectus treatment is non-surgical and involves wearing a bespoke brace or orthosis called a 'Dynamic Chest Compressor', combined with a programme of Yoga exercises that have been developed specifically to augment our non-surgical treatment.
Most NHS trusts no longer recommend surgery for pectus carinatum and pectus carinatum as the conditions are considered to be cosmetic and no threat to physical health.
Our experience and development of custom-made braces has led to many patient success stories.
This depends on several factors; the position of the chest wall deformity, its severity, the flexibility of the chest, the kind of results wanting to be achieved and the age of the person undergoing treatment for pectus excavatum or pectus carinatum.
Early adolescence (roughly between the ages of 12-16 years old) – is an optimum age to start treatment, given that the chest is still maturing, and flexible, permanent correction is more easily achievable. Once bracing treatment is complete and a patient has stopped growing, the deformity will not return. For younger pectus patients, conservative bracing is used to keep a deformity from worsening and can help them to avoid surgery in later life.
For older pectus patients (between the ages of 20 to 30) results can be harder to achieve, as the costal cartilage hardens into the bone as a person matures. Over the years we have successfully treated many adults for both pectus excavatum and pectus carinatum and active adults with flexible chests can expect good results.
Again, this hugely depends on what a patient wants to achieve from treatment; whether that’s avoidance of surgery, improvement in the appearance of the chest shape, reduction in rib flaring etc. All these goals are taken into consideration during your first consultation. While there are no serious health risks of having pectus carinatum or excavatum – beyond the cosmetic – for many patients and parents, treatment outcomes involve improving confidence and self-esteem. During our 2018 Pectus Patient Survey, 92% of pectus carinatum patients surveyed said that treatment had a ‘major improvement’ or ‘an improvement’ on their social life.
You can read the results of our 2018 Pectus Patient Survey and quality of life questionnaire here.
Regular reviews are part of the treatment programme, preferably in clinic with one of our specialist orthotists, or via Skype consultations.
The number of appointments needed will vary from patient to patient but as a general rule, younger pectus patients who are growing at a faster rate will need to be seen more regularly for check-up appointments. This is to ensure that the brace fits well and is guiding the chest into the correct position as growth spurts occur. For other patients, this can be scaled back according to their individual needs and demands.
Regular appointments are beneficial for assessing progress, checking for signs of rubbing and determining whether another brace is needed. Appointments are also good for checking patient compliance to brace wearing and the breathing and exercise programme. At each appointment, we make time for patients to see our physiotherapist to fine-tune their exercise programme and check to see how a patient has been managing with the current programme.
We always advise coming in for appointments whenever you have any concerns about the brace or treatment programme, especially if a brace is rubbing or not fitting correctly. At the London Orthotic Consultancy, we have treated numerous international patients that have benefitted from specially designed braces that leave room to accommodate for growth and that can be adjusted remotely. Follow-up appointments for international patients are conducted via Skype.
This is a very common concern for patients considering treatment; in general, the dynamic chest compressor brace is easy to conceal if you are wearing a loose-fitting shirt for school or work. If you are wearing two chest braces – one for the main deformity and the other for rib flaring – then this may be more noticeable, especially under a t-shirt. Normally loose-fitting clothing will conceal the brace, though it’s likely it will be seen through tight-fitting clothes.
It is really important to continue exercising while going through bracing treatment. Exercise is fundamental to keeping the chest wall flexible. Our treatment programme incorporates a daily exercise routine of around 30-40 minutes of stretching using yoga poses, resistance bands, deep breathing exercises and general muscle stretches. Deep breathing exercises allow the lungs to expand against the chest wall, pushing it outwards.
Exercising with the brace on in the later stages of treatment can also make the chest correction more stable and permanent.
Swimming is one of the best forms of exercise to complement bracing treatment, as the body positions required to swim imitate the resistance band training designed to stretch the chest and increase its flexibility. Some swimming strokes are better for this than others, please check with your clinician. The brace should always be removed for contact sports and for swimming.
For most patients, one brace is often all that is needed to achieve a desired level of correction. They are each designed to last the duration of treatment and accommodate any growth that may occur in that time. Some patients have benefitted from having two braces – one to treat the main deformity and the other to treat rib flaring. For some pectus excavatum patients, having a brace apply pressure to the ribs – in addition to vacuum bell therapy – can greatly reduce the appearance of the depressed sternum area of the chest, forcing it upwards and outwards into a more corrective position.
If you are worried about your chest shape, or your child’s chest shape, then get in touch for a free Skype consultation with one of our pectus specialists who can assess their chest and discuss treatment options. We are always happy to communicate with local GPs, thoracic surgeons and consultants if a patient approaches us for bracing treatment after considering other options.

Mum Natalie shares her experience of having both her identical twins diagnosed with craniosynostosis. Ella and Nina had surgery at Great Ormond Street Hospital before going through cranial remoulding therapy at the London Orthotic Consultancy.

See how a thorough gait analysis and a correctly-fitted, bespoke Reciprocating Gait Orthosis (RGO) helped Ted, a spinal surgery and cancer survivor, improve his rehabilitation and mobility goals, getting him back on his feet again.

We are proud to announce the launch of our latest innovation in non-surgical treatment for pectus deformities. Our new dynamic chest compressor is one of the slimmest pectus braces on the market and is designed to reshape the chest without the need for invasive surgery.

Rosie’s very severe plagiocephaly was no problem for the LOCBand Lite 3D-printed cranial remoulding helmet, going from 16mm to 2mm in just six months.

When John came to see us, his ankle was in a bad way. He had around 60mm of his tibia missing and not much if any talus present. He needed crutches to support him to walk. A gait analysis and a new bespoke carbon fibre knee ankle foot orthosis (KAFO) later and he is able to walk again without crutches.

Matilde travelled from Chile to LOC for bracing treatment for her adolescent idiopathic scoliosis. Now, nearly a year and a half since she started wearing her brace, she has achieved near-total correction of the curvature of her spine. This is her scoliosis bracing story.

After only 6 months of wearing bespoke pectus braces from The London Orthotic Consultancy, Will started to notice a visible difference in his pectus carinatum.

After trying out several scoliosis braces in Romania, Ukraine and Turkey, Iulia begins treatment with the LOC Scoliosis Brace and is already seeing results in a matter of months. Here her mum, Raluca, describes how and why they came to LOC for her treatment.