
19 December 2017
At the London Orthotic Consultancy, we’ve been treating chest wall deformity non-surgically for nearly a decade. We have pioneered bracing as an effective alternative to surgery in the UK. The two main types of congenital chest wall deformity are known as pectus excavatum (when the sternum appears dented inwards) and pectus carinatum (where the sternum protrudes outwards). It’s a complex condition in the way it presents, which can range from mild to severe, mixed type deformity and some people may have an asymmetric deformity too. When the deformity is asymmetrical, it can cause a rotation of the sternum with a slight depression on one side and protrusion on the other.
Our non-surgical treatment follows the dynamic remodelling method, which requires a patient to wear a bespoke orthotic brace known as the dynamic chest compressor, based on a 3D scan and custom made to their exact chest measurements. The brace is gradually adjusted to optimise the direction of force and correction possible. A custom exercise programme is also part of the treatment package and compliance to wearing the brace and carrying out the exercises is key to successful treatment.
No two patients will present in the same way and therefore, degrees of correction and the timeframe in which they can be achieved vary.
Most of our pectus patients are adolescents, though we have had several successful adult pectus patients who have responded well to bracing in part because of their commitment to treatment and the flexibility of their chest. Earlier this year we conducted our inaugural pectus patient survey, of which we are pleased to announce the results.
The average age of patients when treatment began was 16 years old, with treatment time including part-time brace wear in the latter months and continued commitment to the breathing and exercise regime.
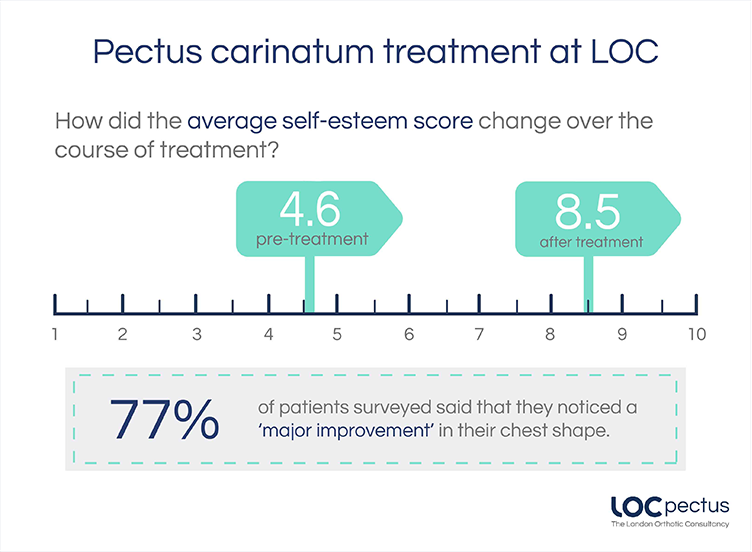
Most pectus patients will not experience any physical complaints, but cosmetic concerns surrounding body image have been associated with low self-esteem and a decreased mental quality of life. Patients who responded to our survey said that their self-esteem score (out of 10) pre-treatment was 4.6, but following treatment, that score went up to 8.5. Consequently, 92% of patients said that treatment had made a ‘major improvement’ or ‘an improvement’ to their social life – incredible news for both patients and clinicians, particularly as this has meant invasive corrective surgery could be avoided.
For patients who experience rib flaring, where their chest deformity causes the ribs to protrude slightly, they will often require a second dynamic chest compressor. We have achieved excellent results with the rib flaring brace alone, which can also be used post-surgery in some cases. Out of those patients who did have a second brace, 94% said it helped with their rib flaring.
Excavatum can be slightly more difficult to treat, given that the use of the vacuum bell relies on a negative force to lift the sternum up and out (as opposed to the downward pressure exerted by the carinatum dynamic chest compressor).
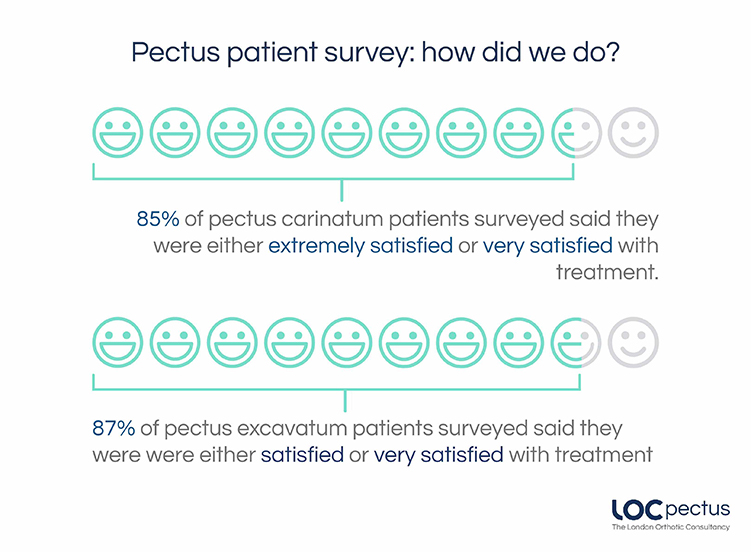
Out of those surveyed, 87% of patients surveyed were either ‘satisfied’ or ‘very satisfied' with treatment, with 75% saying that their chest appearance improved following treatment.
70% of pectus excavatum patients said that they would recommend LOC’s treatment to a friend.
If you would like to book an appointment with a pectus clinician, call our clinic on 020 8974 9989. The initial consultation is FREE with no obligation to proceed.
Rewardingly, 77% of pectus carinatum patients said they noticed a ‘major improvement’ in their chest shape, with another 15% saying it had ‘improved’. While 85% of patients surveyed were either ‘extremely’ or ‘very satisfied' with the treatment, 92% said that they would recommend treatment to a friend.
This depends on several factors; the position of the chest wall deformity, its severity, the flexibility of the chest, the kind of results wanting to be achieved and the age of the person undergoing treatment for pectus excavatum or pectus carinatum.
Early adolescence (roughly between the ages of 12-16 years old) – is an optimum age to start treatment, given that the chest is still maturing, and flexible, permanent correction is more easily achievable. Once bracing treatment is complete and a patient has stopped growing, the deformity will not return. For younger pectus patients, conservative bracing is used to keep a deformity from worsening and can help them to avoid surgery in later life.
For older pectus patients (between the ages of 20 to 30) results can be harder to achieve, as the costal cartilage hardens into the bone as a person matures. Over the years we have successfully treated many adults for both pectus excavatum and pectus carinatum and active adults with flexible chests can expect good results.
Again, this hugely depends on what a patient wants to achieve from treatment; whether that’s avoidance of surgery, improvement in the appearance of the chest shape, reduction in rib flaring etc. All these goals are taken into consideration during your first consultation. While there are no serious health risks of having pectus carinatum or excavatum – beyond the cosmetic – for many patients and parents, treatment outcomes involve improving confidence and self-esteem. During our 2018 Pectus Patient Survey, 92% of pectus carinatum patients surveyed said that treatment had a ‘major improvement’ or ‘an improvement’ on their social life.
You can read the results of our 2018 Pectus Patient Survey and quality of life questionnaire here.
Regular reviews are part of the treatment programme, preferably in clinic with one of our specialist orthotists, or via Skype consultations.
The number of appointments needed will vary from patient to patient but as a general rule, younger pectus patients who are growing at a faster rate will need to be seen more regularly for check-up appointments. This is to ensure that the brace fits well and is guiding the chest into the correct position as growth spurts occur. For other patients, this can be scaled back according to their individual needs and demands.
Regular appointments are beneficial for assessing progress, checking for signs of rubbing and determining whether another brace is needed. Appointments are also good for checking patient compliance to brace wearing and the breathing and exercise programme. At each appointment, we make time for patients to see our physiotherapist to fine-tune their exercise programme and check to see how a patient has been managing with the current programme.
We always advise coming in for appointments whenever you have any concerns about the brace or treatment programme, especially if a brace is rubbing or not fitting correctly. At the London Orthotic Consultancy, we have treated numerous international patients that have benefitted from specially designed braces that leave room to accommodate for growth and that can be adjusted remotely. Follow-up appointments for international patients are conducted via Skype.
This is a very common concern for patients considering treatment; in general, the dynamic chest compressor brace is easy to conceal if you are wearing a loose-fitting shirt for school or work. If you are wearing two chest braces – one for the main deformity and the other for rib flaring – then this may be more noticeable, especially under a t-shirt. Normally loose-fitting clothing will conceal the brace, though it’s likely it will be seen through tight-fitting clothes.
It is really important to continue exercising while going through bracing treatment. Exercise is fundamental to keeping the chest wall flexible. Our treatment programme incorporates a daily exercise routine of around 30-40 minutes of stretching using yoga poses, resistance bands, deep breathing exercises and general muscle stretches. Deep breathing exercises allow the lungs to expand against the chest wall, pushing it outwards.
Exercising with the brace on in the later stages of treatment can also make the chest correction more stable and permanent.
Swimming is one of the best forms of exercise to complement bracing treatment, as the body positions required to swim imitate the resistance band training designed to stretch the chest and increase its flexibility. Some swimming strokes are better for this than others, please check with your clinician. The brace should always be removed for contact sports and for swimming.
For most patients, one brace is often all that is needed to achieve a desired level of correction. They are each designed to last the duration of treatment and accommodate any growth that may occur in that time. Some patients have benefitted from having two braces – one to treat the main deformity and the other to treat rib flaring. For some pectus excavatum patients, having a brace apply pressure to the ribs – in addition to vacuum bell therapy – can greatly reduce the appearance of the depressed sternum area of the chest, forcing it upwards and outwards into a more corrective position.
If you are worried about your chest shape, or your child’s chest shape, then get in touch for a free Skype consultation with one of our pectus specialists who can assess their chest and discuss treatment options. We are always happy to communicate with local GPs, thoracic surgeons and consultants if a patient approaches us for bracing treatment after considering other options.